
|
시장보고서
상품코드
2063732
이식 약물 모니터링 검사 치료 : 시장 점유율 분석, 업계 동향 및 통계, 성장 예측(2026-2031년)Transplant Drug Monitoring Assay Treatment - Market Share Analysis, Industry Trends & Statistics, Growth Forecasts (2026 - 2031) |
||||||
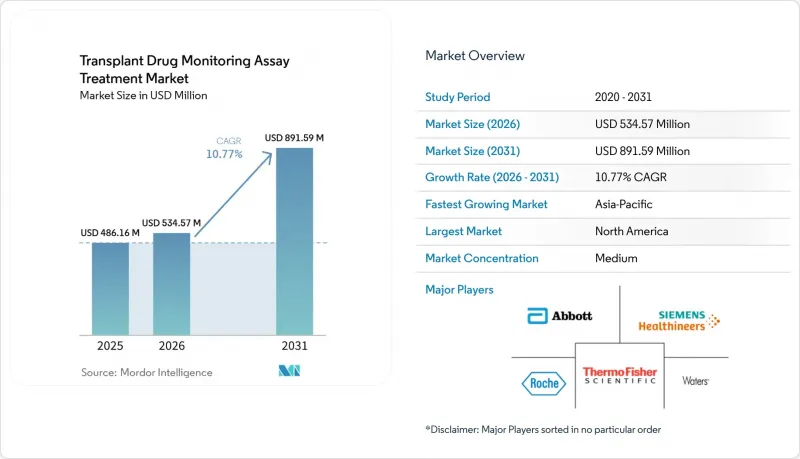
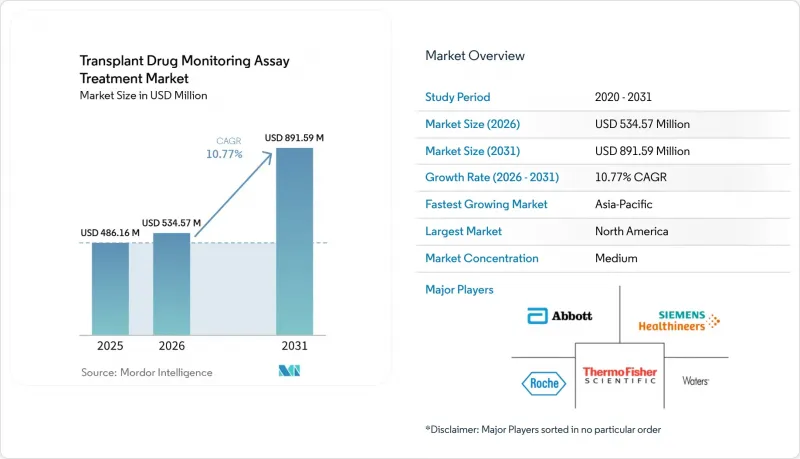
Mordor Intelligence에 의하면, 이식 약물 모니터링 검사 치료 시장 규모는 2025년에 4억 8,616만 달러로 평가되었습니다. 2026년에 5억 3,457만 달러에서 2031년까지 8억 9,159만 달러에 이를 것으로 예측되며, 2026-2031년 CAGR은 10.77%를 나타낼 전망입니다.
본 보고서는 약물 또는 분석 대상 물질의 유형(칼시뉴린 억제제 등), 기술(면역측정법, LC-MS/MS), 최종 사용자(병원 및 이식 센터의 검사실 등), 이식 유형(신장, 간 등), 지역(북미, 유럽, 아시아태평양, 중동 및 아프리카, 남미)별로 분류되어 있습니다. 시장 전망은 달러 기준 금액으로 제시되어 있습니다.
세계의 이식 약물 모니터링 검사 치료 시장 동향 및 인사이트
장기 이식 건수 증가가 TDM 수요를 뒷받침하고 있습니다.
2024년 전 세계 고형 장기 이식 건수는 17만 3,727건에 달하고, 2023년 대비 2% 증가했습니다. 또한, 신장 및 간 이식 건수는 평생에 걸쳐 면역억제제의 투여를 모니터링해야 하는 수술군 중에서 여전히 가장 큰 비중을 차지하고 있습니다. 미국에서는 2024년에 4만 8,000건 이상의 이식이 이루어졌으며, 국내 대기자 명단은 10만 3,000명을 계속 넘어서는 상황입니다. 이는 이식 전 및 이식 후 각 단계에서 일관된 약물 노출 모니터링에 대한 지속적인 수요가 있음을 보여줍니다. 스페인은 인구 100만 명당 53.93명의 사체 장기 기증자 수를 기록하며, 사체 장기 기증 분야에서 1위를 차지했습니다. 한편, 튀르키예와 사우디아라비아는 각각 100만 명당 50명을 넘는 생체 장기 기증자 수를 기록했으며, 이는 의료 시스템 전반의 검사 건수나 플랫폼 구성을 좌우하는 지역 간 격차가 뚜렷이 드러났음을 보여줍니다. 조혈모세포 이식 프로그램에서는 이식 후 초기 단계의 검사 빈도가 증가하고 있으며, 동종 이식을 받은 환자의 이식편 대 숙주 질환(GVHD) 위험을 관리하기 위해 타크롤리무스의 최저 농도 모니터링이 강화되고 있습니다. 2025년 연구에 따르면, 조혈모세포이식(HSCT) 후 1-4주 동안 타크로리무스의 치료 범위 내 유지율을 75.9% 이상 유지하는 것이 2-3등급 급성 GVHD의 감소와 상관관계가 있는 것으로 나타났으며, 중요한 초기 단계에서 정확하고 빈번한 트로프 모니터링의 필요성이 입증되었습니다.
칼시뉴린 억제제 지침에 따른 모니터링
타크로리무스의 트래프 농도 모니터링은 고형 장기 및 줄기세포 이식의 치료 경로에 포함되어 있으며, 거부 반응이나 독성을 유발할 수 있는 약물 노출 부족이나 과다 노출을 방지하기 위해, 국내 프로토콜에서는 이식 후 6개월 동안 정기적인 모니터링 빈도가 규정되어 있습니다. 2025년 다기관 비교 연구에서 동일 환자에 대한 타크롤리무스의 면역측정법과 LC-MS/MS 결과를 비교했을 때, 이식 후 3개월 이내에는 28%, 3개월 이후에는 37%라는 임상적으로 의미 있는 불일치가 보고되었으며, 이는 임상 현장에서 재검 전략 및 환자별 측정법의 일관성이 중요한 이유를 뒷받침하고 있습니다. 최신 LC-MS/MS법에서는 특정 시행 조건 하에서 면역측정법과 비교하여 약 7.5%에서 18.7%의 체계적인 음의 편향이 확인되고 있으며, 구식 면역측정법에 근거하여 설정된 치료 목표치를 변경하지 않고 질량분석 결과에 적용할 경우, 무의식적인 투여 부족을 초래할 가능성이 있습니다. 스코틀랜드 국민보건서비스(NHS Scotland)의 지침에 따르면, 첫 6개월 동안 타크로리무스의 월별 최저 농도가 설정되어 있으며, 전문의의 감독 하에 투여량 조정이 이루어집니다. 이를 통해 1차 진료에서 발생하는 오해를 줄이고, 투여량이 안정화될 때까지의 기간 동안 검사 빈도를 표준화할 수 있게 됩니다. 규제 측면의 진전에 따라 자동화된 LC-MS/MS 플랫폼이 중간 수준의 복잡도를 지닌 CLIA 분류로 전환되었고, IVDR 클래스 C 인증을 통해 키트의 입수 가능성이 확대됨에 따라 임상 실험실의 업무 부담이 경감되었습니다. 이를 통해 워크플로우를 지침 준수와 대규모로 연계할 수 있게 됩니다. 최근의 동료 심사를 거친 평가에서 분석법의 편향성이나 교정 관행이 지적된 바와 같이, 불일치 사례에 대해 백업 수단으로 LC-MS/MS를 병용하는 경우, 시판되는 표준화된 면역 분석법은 일상적인 모니터링에서 여전히 허용됩니다.
면역측정법의 교차반응성 또는 편향 대 LC-MS/MS의 특이성
특정 타크로리무스 면역분석법은 대사산물과 교차반응을 일으킬 가능성이 있어, 특정 임상 상황에서 결과가 과대평가될 우려가 있으며, 임상 상황과 측정값이 일치하지 않을 경우 재검사가 필요합니다. 비교 평가 결과, 서로 다른 면역 측정법에서 비례적인 양성 편향이 보고되었으나, Abbott Alinity i와 같은 새로운 플랫폼에서는 편향이 LC-MS/MS의 벤치마크 값에 가까워져, 이를 통해 저농도 표적에 대한 신뢰성이 향상되었습니다. 검사 건수가 많은 검사실의 운영 평가에 따르면, LC-MS/MS에서 최신 면역측정법으로 전환함으로써 대부분의 검체에 대해 분석 결과의 일관성을 유지하면서 검사 소요 시간을 단축할 수 있는 것으로 나타났습니다. 다만, 여전히 일정 수의 검체는 LC-MS/MS의 신뢰 구간 밖으로 나타나므로 후속 조치가 필요합니다. 이식 후 초기 용량 조절 단계에서는 의사가 단기간의 미세한 변동을 바탕으로 조치를 취하는 경우가 많기 때문에 측정값의 편향으로 인한 임상적 위험이 높아집니다. LC-MS/MS는 대사산물의 간섭 문제를 해결해 주지만, 그 대신 분석법 설정이 복잡해지고 실험실 간 편차가 발생한다는 과제가 있습니다. 따라서 결과에 따라 투여량을 자주 조정해야 하는 경우, 표준화된 키트와 교정기의 가치가 더욱 높아집니다.
부문별 분석
칼시뉴린 억제제는 신장, 간, 심장, 폐 및 줄기세포 이식 프로토콜에서 1차 선택 약물로 사용되는 역할을 바탕으로, 2025년 이식 약물 모니터링 검사 치료 시장 규모의 45.08%를 차지했습니다. 타크로리무스는 신장 이식 환자의 면역 억제 요법의 핵심이며, 미국에서는 환자의 90% 이상에게 사용되고 있습니다. 이는 이식 직후부터 장기 유지 요법에 이르기까지 빈번한 검사가 필요함을 의미합니다. 이식 직후 모니터링 빈도가 높고, 특정 장기의 경우 치료 범위가 좁아야 하기 때문에 검사 수요가 높은 수준을 유지하고 있으며, 이것이 칼시뉴린 억제제가 시장 전체에서 주도적인 점유율을 차지하는 요인이 되고 있습니다. 차세대 면역 측정법의 편향이 감소함에 따라, 표준 타크로리무스 목표치 부근에서 LC-MS/MS와의 일치도가 향상되었습니다. 이를 통해 결과와 임상 소견에 불일치가 있을 경우 LC-MS/MS로 선택적으로 리플렉스 검사를 실시함으로써, 병원 검사실이 신속 면역 분석법에 대한 의존도를 유지하고 있습니다. 유지 요법 단계에서 3-5 ng/mL를 목표로 하는 CNI 최소화 프로토콜에서는 범위 하한선에서의 용량 조절에 있어 LC-MS/MS의 정확도가 중요시되고 있으며, 이를 통해 CNI가 1차 선택 약제로서의 위상을 잃지 않으면서도 질량 분석법의 역할이 커지고 있습니다.
mTOR 억제제는 CNI 관련 신독성을 보이는 환자의 신기능을 보호하는 대체 전략에 힘입어, 2031년까지 연평균 성장률(CAGR) 11%를 나타낼 것으로 전망됩니다. 임상시험 결과를 통해 특정 환자군에서 시롤리무스로 전환한 후 신기능이 개선된 것으로 확인되었으며, 이는 상태가 안정된 수혜자를 대상으로 한 일상 진료에서 프로토콜에 따른 전환의 근거가 되고 있습니다. 에베롤리무스와 저용량 타크롤리무스의 병용 요법은 임상시험에서 eGFR의 예후를 유지하면서 바이러스 감염률을 낮추는 데 성공했으며, 이를 통해 바이러스 감염 위험이 높은 환경에서 mTOR 억제제의 유용성이 확대되고 있습니다. 부작용이나 수술 부위에 대한 우려로 인한 투여 중단률은 여전히 도입을 제한하고 있지만, 임상의들이 신장 기능 위험이나 감염 이력에 따라 치료 요법을 조정함에 따라 이 약물군은 호조를 유지하고 있습니다. 미코페놀산 등의 항대사제는 여전히 일상적인 TDM(치료 약물 모니터링)이 시행되지 않는 병용 요법이며, 이로 인해 검사 건수에 미치는 직접적인 영향이 제한되고 있습니다. 이식 약물 모니터링 분석법 분야는 CNI(칼시모듈린 억제제)의 사용 최소화 및 mTOR로의 전환 프로토콜이 복잡해지는 등 치료 방식의 변화를 반영하고 있으며, 저농도 영역에서의 정량 및 장기간에 걸친 측정법의 일관성이 요구되기 때문에 LC-MS/MS가 선호되고 있습니다.
2025년 기준으로, 면역 분석 플랫폼은 이식 약물 모니터링 검사 치료 시장의 56.13% 점유율을 차지했습니다. 이는 병원 검사실이 15분에서 60분의 처리 시간을 목표로 하며, 화학 검사 워크플로우에 부합하는 완전 자동화된 운영을 우선시하기 때문입니다. 새로운 시스템에서는 편향 성능이 개선되어 빈번한 확인 검사의 필요성이 줄어들었으며, 이식 후 초기 단계에서 신속한 투여량 조정 주기를 지원합니다. 지멘스의 ACMIA 도입으로 1 ng/mL의 감도에서 15분 이내에 결과를 얻을 수 있게 되어, 면역측정을 우선하는 방식을 유지하고 있는 기관에서 긴급 검사를 위한 실용적인 대안이 되고 있습니다. 이종 항체나 드문 교차 반응 현상에 대처하기 위해서는 여전히 전처리 및 간섭 관리 프로토콜이 필요하며, 검사실에서는 필요에 따라 예상치 못한 결과에 대해 LC-MS/MS를 이용한 재검사를 실시함으로써 이를 완화하고 있습니다.
LC-MS/MS는 표준화된 키트 기반 솔루션을 통해 방법 개발 및 검증에 드는 업무 부담이 줄어들 것으로 예상에 따라, 2031년까지 연평균 성장률(CAGR) 11.3%를 나타낼 것으로 전망됩니다. 2024년 12월에 출시된 로슈(Roche)사의 cobas Mass Spec 솔루션과, 그 후 면역억제제 및 항생제에 이르는 검사 항목의 확충을 통해, 기존에는 면역측정법에 의존하던 일상 검사실에도 자동 질량 분석이 도입되어 기준 수준의 특이도를 확보할 수 있게 되었습니다. 시마즈 제작소의 IVDR 클래스 C ‘DOSIMMUNE’ 키트는 모든 시약과 검증된 방법을 한 세트로 구성함으로써, 검체당 총 분석 시간을 단축하고, 구매부터 임상 운용 개시까지의 기간을 더욱 단축합니다. 세계 계량 표준 체계에 대한 추적성을 갖춘 교정기는 시설 간 비교 가능성을 높이며, 유지 요법 프로토콜에서 치료 목표치가 좁아지거나 낮은 수치를 보이는 경우, LC-MS/MS의 장기적인 도입 근거를 강화합니다. 따라서, 이식 약물 모니터링 검사 치료 업계에서는 긴급 상황의 요구에 대응할 수 있는 신속한 면역 분석법과, 확인 검사 및 저농도 표적에 적합한 LC-MS/MS 간의 균형을 맞추고 있으며, 이를 통해 병원과 검사 기관을 아우르는 하이브리드 검사 모델이 뒷받침되고 있습니다.
지역별 분석
북미는 2025년에 51.11%의 점유율을 유지했습니다. 이는 이식 건수가 많고, 병원 검사실의 수용 능력이 광범위하며, 자동화 LC-MS/MS 플랫폼이 적극적으로 도입됨에 따라 면역 분석법과 질량 분석법 모두에 대한 수요가 증가했기 때문입니다. 미국에서는 2024년에 4만 8,000건 이상의 이식이 이루어졌으며, 10만 3,000명이 넘는 후보자가 등록된 전국 대기 명단으로 인해 치료 전 과정에 걸친 타크롤리무스의 정밀 모니터링에 대한 수요가 지속되고 있습니다. FDA 승인을 받은 면역 분석법과 주요 진단기기 제조업체들이 도입한 자동화 질량 분석 메뉴의 확충을 통해 분석 성능과 워크플로우의 표준화가 향상되어, 임상 실험실의 업무 부담이 경감되고 있습니다. 이 지역에서 모델 기반의 정밀 투약을 시행한 연구에 따르면, 전자건강기록(EHR)에 통합된 알고리즘을 통해 조기 목표 달성률이 향상된 것으로 나타났으며, 이는 해당 지역이 중시하는 상호운용성과 임상 의사결정 지원의 경향과 부합합니다.
유럽은 2025년 전 세계 매출의 상당 부분을 차지했으며, 면역억제제 검사를 C등급으로 지정하고 검증 기준을 강화하는 EU IVDR(체외진단용 의료기기 규정)에 따라 지속적인 발전을 거듭하고 있습니다. IVDR 인증을 획득한 LC-MS/MS 키트와 CE 마크를 획득한 자동 질량 분석 시스템을 통해, EU 내 실험실에서 선택할 수 있는 표준화된 옵션이 확대되었으며, 시설 간에 더욱 일관된 성능이 보장되고 있습니다. 스페인은 해당 지역에서 사후 장기 기증률이 가장 높으며, 이는 1인당 이식 건수가 높은 수준을 유지하는 데 기여하고 있어, 이에 따라 전국의 이식 센터에서 신뢰성이 높은 TDM에 대한 수요가 증가하고 있습니다. 유럽 이식 학회의 지침에서는 표준 범위에 대해서는 면역측정법을 유지하면서, 타크롤리무스의 저농도 목표치에 대해서는 LC-MS/MS를 권장함으로써 비용과 정확도의 균형을 맞추고 있으며, 이를 통해 임상 현장에서의 하이브리드 검사 전략이 강화되고 있습니다.
아시아태평양에서는 이식 프로그램의 확대와 정부의 이식 후 모니터링 접근성 확대에 힘입어, 2031년까지 연평균 성장률(CAGR) 11.5%를 나타낼 것으로 전망됩니다. 인프라 확충과 중앙 검사실 네트워크 구축에 힘입어 도시 지역에서 LC-MS/MS 도입이 진행되고 있지만, 대부분의 병원에서는 응급 검사 시 면역 측정을 우선시하는 방식이 여전히 일반적입니다. 유럽 및 아시아에서 마이크로 샘플링 도입에 관한 연구 결과, 환자들의 강력한 지지가 확인되었으며, 상온 운송이 가능해짐에 따라 콜드체인 물류가 제한되는 상황에서도 지방 및 외딴 지역으로의 서비스 제공 범위를 확대할 수 있습니다. 중동에서는 이식 건수가 많은 병원들이 분석 성능을 강화하고 수동 방식에 대한 의존도를 줄이기 위해 자동화된 LC-MS/MS를 도입하고 있으며, 이는 자원이 허용하는 한 지역 전체적으로 표준화된 플랫폼으로의 전환이 진행되고 있음을 보여줍니다. 남미에서는 주요 도시의 병원에서 특정 TDM 검사에 대한 공적 보험 적용이 검사 접근성을 높이고 있는 반면, 병원이 면역측정법을 통한 긴급 검사 능력을 유지하는 가운데, 보다 복잡한 검사는 지역 기준 검사 기관이 담당하고 있습니다. 지역을 불문하고, 이식 약물 모니터링 검사·치료 시장에서는 병상에서의 신속한 면역 측정과, 확인 검사 및 저농도 표적에 대한 표준화된 LC-MS/MS를 중심으로 한 하이브리드 검사의 도입이라는 일관된 추세가 나타나고 있습니다.
기타 혜택 :
- 엑셀 형식 시장 예측(ME) 시트
- 3개월간의 애널리스트 지원
자주 묻는 질문
목차
제1장 서론
제2장 조사 방법
제3장 주요 요약
제4장 시장 구도
제5장 시장 규모 및 성장 예측(금액;주요 분석 항목 수량)
제6장 경쟁 구도
제7장 시장 기회 및 향후 전망
KTH 26.06.24According to Mordor Intelligence, the transplant drug monitoring assay treatment market size is projected to be USD 486.16 million in 2025, USD 534.57 million in 2026, and reach USD 891.59 million by 2031, growing at a CAGR of 10.77% from 2026 to 2031.
This report is Segmented by Drug or Analyte Class (Calcineurin Inhibitors, and More), Technology (Immunoassay, LC-MS/MS), End User (Hospital and Transplant Center Laboratories, and More), Transplant Type (Kidney, Liver, and More), and Geography (North America, Europe, Asia-Pacific, Middle East and Africa, South America). Market Forecasts are Provided in Terms of Value in USD.
Global Transplant Drug Monitoring Assay Treatment Market Trends and Insights
Rising Organ Transplant Volumes Sustain TDM Demand
Global solid organ transplant activity reached 173,727 in 2024, a 2% increase from 2023, and kidney and liver volumes continued to represent the largest procedure cohorts that require lifelong therapeutic drug monitoring of immunosuppressants. In the United States, more than 48,000 transplants were performed in 2024, and the national waiting list remained above 103,000 candidates, which signals durable demand for consistent drug exposure monitoring across pre- and post-transplant phases . Spain led deceased organ donation at 53.93 donors per million people, while Turkey and Saudi Arabia each exceeded 50 living donors per million, highlighting regional differences that shape testing volumes and platform mix across health systems. Hematopoietic stem cell transplant programs have raised testing frequency in the early post-transplant period, which intensifies tacrolimus trough-level monitoring to manage graft-versus-host disease risk in allogeneic recipients. A 2025 study showed that maintaining tacrolimus time-in-therapeutic-range at or above 75.9% during weeks 1 to 4 post-HSCT correlated with reduced Grade II-III acute GVHD, reinforcing the need for precise and frequent trough monitoring in critical early windows.
Guideline-Mandated Monitoring of Calcineurin Inhibitors
Tacrolimus trough monitoring is embedded in care pathways for solid organ and stem cell transplantation, and national protocols specify routine frequency in the first 6 months to avoid underexposure or overexposure that can lead to rejection or toxicity. A 2025 multi-center comparison reported clinically relevant discrepancies of 28% within the first 3 months and 37% after 3 months when comparing immunoassay and LC-MS/MS tacrolimus results in the same patients, which underscores why confirmatory strategies and consistent method use for each patient matter in practice . Modern LC-MS/MS methods have shown systematic negative bias of roughly 7.5% to 18.7% relative to immunoassays in certain implementations, which can create silent underdosing if therapeutic targets calibrated to older immunoassays are applied unchanged to mass-spectrometry results. NHS Scotland guidance sets monthly tacrolimus trough levels for the first 6 months with dose adjustments maintained under specialist oversight, which helps reduce misinterpretation in primary care and standardizes frequency during dose stabilization. Regulatory progress has reduced complexity in clinical labs as automated LC-MS/MS platforms moved into moderate-complexity CLIA categorization and IVDR Class C certifications expanded kit availability, which helps align workflows with guideline adherence at scale. Commercially harmonized immunoassays remain acceptable for routine monitoring when paired with backup LC-MS/MS for discordant cases, as highlighted by recent peer-reviewed assessments of assay bias and calibration practices.
Immunoassay Cross-Reactivity or Bias Versus LC-MS/MS Specificity
Certain tacrolimus immunoassays can cross-react with metabolites, which can inflate results under specific clinical conditions and necessitate reflex testing when clinical context and measured levels diverge. Comparative evaluations have reported proportional positive bias for different immunoassays, although newer platforms such as Abbott Alinity i have reduced bias closer to LC-MS/MS benchmarks, which improves reliability at lower trough targets. Operational assessments from high-volume labs show that switching from LC-MS/MS to a modern immunoassay can cut turnaround time while maintaining analytical agreement for most samples, though a meaningful minority still fall outside LC-MS/MS confidence intervals and need follow-up. Early post-transplant dose titration intervals amplify the clinical risk from biased readings because physicians often act on narrow deltas in short time frames. LC-MS/MS resolves metabolite interference but introduces its own method setup complexity and interlaboratory variability, which reinforces the value of standardized kits and calibrators when results drive frequent dosing changes.
Other drivers and restraints analyzed in the detailed report include:
- Broader Analyzer Menus and Kit Availability for Immunoassays
- Standardized, Kit-Based LC-MS/MS Improves Adoption and Comparability
- Skilled-Staff Shortages and LC-MS/MS Complexity Slow Adoption
For complete list of drivers and restraints, kindly check the Table Of Contents.
Segment Analysis
Calcineurin inhibitors accounted for 45.08% of the Transplant Drug Monitoring Assay Treatment market size in 2025 based on their first-line role in kidney, liver, heart, lung, and stem cell transplantation protocols. Tacrolimus remains the backbone of immunosuppression in kidney recipients and is used in more than 90% of cases in the United States, which translates into high assay frequency from the immediate post-transplant period to long-term maintenance . The higher frequency of early-life monitoring and the need for narrow therapeutic ranges in select organs keep testing intense, which supports the leading share of calcineurin inhibitors within the overall mix. Lower bias on next-generation immunoassays has improved alignment with LC-MS/MS near standard tacrolimus targets, which sustains hospital lab reliance on fast immunoassays with selective reflex to LC-MS/MS when results and the clinical picture conflict. CNI-minimization protocols that target 3 to 5 ng/mL in the maintenance phase favor LC-MS/MS precision for dose titration at the low end of the range, which elevates the role of mass spectrometry without displacing the first-line status of CNIs.
mTOR inhibitors are projected to grow at 11% CAGR through 2031, supported by conversion strategies that protect renal function in patients with CNI-related nephrotoxicity. Evidence from clinical studies has documented renal function gains after sirolimus conversion in select patient profiles, which underpins protocolized switches in routine care for stable recipients. Everolimus paired with reduced-dose tacrolimus achieved lower viral infection rates in trials while maintaining eGFR outcomes, which broadens mTOR inhibitor appeal in high-viral-risk settings. Discontinuation rates due to adverse events and surgical wound concerns continue to limit adoption, yet the therapy class remains on a positive trajectory as clinicians tailor regimens by renal risk and infection history. Antimetabolites such as mycophenolic acid remain co-therapies without routine TDM, which caps their direct impact on assay volume. The Transplant Drug Monitoring Assay Treatment industry reflects these therapy shifts through rising complexity of CNI minimization and mTOR conversion protocols, which favor LC-MS/MS for low-range quantification and method consistency over time.
Immunoassay platforms held 56.13% share of the Transplant Drug Monitoring Assay Treatment market size in 2025, as hospital labs prioritize 15 to 60 minute turnaround times and fully automated operations that align with chemistry workflows. Bias performance has improved on newer systems, which reduces the need for frequent confirmatory testing and supports rapid dose adjustment cycles during the early post-transplant period. Siemens' ACMIA implementation delivers sub-15-minute results at 1 ng/mL sensitivity, which positions it as a practical option for stat testing in centers that maintain immunoassay-first pathways. Pre-analytical and interference management protocols remain necessary to address heterophilic antibodies and rare cross-reactivity events, which labs mitigate by retesting unexpected values with LC-MS/MS when appropriate.
LC-MS/MS is projected to expand at 11.3% CAGR through 2031 as standardized, kit-based solutions reduce method development and verification workloads. Roche's cobas Mass Spec solution, launched in December 2024, and subsequent menu expansions across immunosuppressants and antibiotics brought automated mass spectrometry into routine labs that historically relied on immunoassays, which increases access to reference-quality specificity. Shimadzu's IVDR Class C DOSIMMUNE kit reduces total analysis time per sample while bundling all reagents and validated methods, which further shortens the path from purchase to clinical go-live. Calibrators with traceability from global metrology frameworks enhance cross-site comparability, which strengthens the long-term case for LC-MS/MS when therapeutic targets are narrow or trending lower in maintenance protocols. The Transplant Drug Monitoring Assay Treatment industry is therefore balancing fast-turnaround immunoassays for stat needs with LC-MS/MS for confirmatory and low-range targets, which supports a hybrid testing model across hospital and reference laboratories.
Geography Analysis
North America retained 51.11% share in 2025 as high transplant volumes, broad hospital lab capacity, and active adoption of automated LC-MS/MS platforms reinforced demand for both immunoassay and mass-spec testing. The United States performed more than 48,000 transplants in 2024, and a national waiting list exceeding 103,000 candidates sustains ongoing demand for precise tacrolimus monitoring across the care continuum. FDA-cleared immunoassays and expanding automated mass-spec menus introduced by major diagnostics companies have improved analytical performance and workflow standardization, which reduces the operational burden on clinical labs. Studies implementing model-informed precision dosing in this region have shown better early target attainment with EHR-embedded algorithms, which aligns with the region's emphasis on interoperability and clinical decision support.
Europe accounted for a significant portion of global revenues in 2025 and continues to evolve under the EU IVDR regime, which designates immunosuppressant tests as Class C and raises validation rigor. IVDR-certified LC-MS/MS kits and CE-marked automated mass-spectrometry systems have broadened standardized options for EU laboratories, which supports more consistent performance across sites. Spain leads deceased donation rates in the region, which helps sustain higher per-capita transplant activity and the associated need for reliable TDM at transplant centers nationwide. Guidance from European transplant societies balances cost considerations with accuracy by recommending LC-MS/MS for lower tacrolimus targets while preserving immunoassays for standard ranges, which reinforces hybrid testing strategies in clinical practice.
Asia Pacific is projected to grow at 11.5% CAGR through 2031 as transplant programs scale and governments broaden access to post-transplant monitoring. Infrastructure expansion and centralized reference laboratory networks support the roll-out of LC-MS/MS capacity in urban centers, while immunoassay-first models remain the norm for stat testing in most hospitals. Microsampling adoption studies in Europe and Asia point to strong patient preference and enable ambient shipping, which can extend reach into rural and remote settings even when cold-chain logistics are constrained. In the Middle East, high-volume transplant hospitals are deploying automated LC-MS/MS to strengthen analytical performance and reduce reliance on manual methods, which signals a region-wide shift toward standardized platforms where resources permit. In South America, public insurance coverage for select TDM tests at major urban hospitals supports access, while regional reference labs absorb more complex testing as hospitals maintain immunoassay stat capacity. Across regions, the Transplant Drug Monitoring Assay Treatment market reflects a consistent pattern of hybrid testing adoption, anchored by fast immunoassays near the bedside and standardized LC-MS/MS for confirmatory and low-range targets.
- Abbott Laboratories
- Roche
- Siemens Healthineers
- Thermo Fisher Scientific (Microgenics)
- Tosoh
- Sekisui Medical
- Snibe
- Chromsystems
- RECIPE Chemicals + Instruments
- Waters Corporation
- Agilent Technologies
- SCIEX
- Shimadzu Chemistry & Diagnostics
- Bruker (Daltonics)
- Zivak Technologies
- Randox Laboratories
Additional Benefits:
- The market estimate (ME) sheet in Excel format
- 3 months of analyst support
TABLE OF CONTENTS
1 Introduction
- 1.1 Study Assumptions & Market Definition
- 1.2 Scope of the Study
2 Research Methodology
3 Executive Summary
4 Market Landscape
- 4.1 Market Overview
- 4.2 Market Drivers
- 4.2.1 Rising organ transplant volumes sustain TDM demand
- 4.2.2 Guideline-mandated monitoring of calcineurin inhibitors
- 4.2.3 Broader analyzer menus and kit availability for immunoassays
- 4.2.4 Standardized, kit-based LC-MS/MS improves adoption and comparability
- 4.2.5 AI/Bayesian dosing workflows embedding TDM in clinical decision support
- 4.2.6 Microsampling and home-based collections increase test accessibility
- 4.3 Market Restraints
- 4.3.1 Immunoassay cross-reactivity/bias versus LC-MS/MS specificity
- 4.3.2 Skilled-staff shortages and LC-MS/MS complexity slow adoption
- 4.3.3 Belatacept and other non-TDM regimens reduce test volumes in select centers
- 4.3.4 Inter-method variability and lack of harmonized ranges hinder switching
- 4.4 Value / Supply-Chain Analysis
- 4.5 Regulatory Landscape
- 4.6 Technological Outlook
- 4.7 Porters Five Forces
- 4.8 External Quality Assessment (EQA) Trends
5 Market Size & Growth Forecasts (Value; volume for key analytes)
- 5.1 By Drug/Analyte Class
- 5.1.1 Calcineurin inhibitors
- 5.1.2 mTOR inhibitors
- 5.1.3 Antimetabolites
- 5.2 By Technology
- 5.2.1 Immunoassay
- 5.2.2 LC-MS/MS
- 5.3 By End User
- 5.3.1 Hospital & Transplant Center Laboratories
- 5.3.2 Reference/Independent Laboratories
- 5.3.3 Academic & Research Laboratories
- 5.4 By Transplant Type
- 5.4.1 Kidney
- 5.4.2 Liver
- 5.4.3 Heart
- 5.4.4 Lung
- 5.4.5 Hematopoietic Stem Cell Transplant (HSCT)
- 5.5 By Geography
- 5.5.1 North America
- 5.5.1.1 United States
- 5.5.1.2 Canada
- 5.5.1.3 Mexico
- 5.5.2 Europe
- 5.5.2.1 Germany
- 5.5.2.2 United Kingdom
- 5.5.2.3 France
- 5.5.2.4 Italy
- 5.5.2.5 Spain
- 5.5.3 Asia-Pacific
- 5.5.3.1 China
- 5.5.3.2 India
- 5.5.3.3 Japan
- 5.5.3.4 South Korea
- 5.5.3.5 Australia
- 5.5.3.6 Rest of Asia-Pacific
- 5.5.4 Middle East & Africa
- 5.5.4.1 GCC
- 5.5.4.2 South Africa
- 5.5.4.3 Rest of Middle East and Africa
- 5.5.5 South America
- 5.5.5.1 Brazil
- 5.5.5.2 Argentina
- 5.5.5.3 Rest of South America
- 5.5.1 North America
6 Competitive Landscape
- 6.1 Market Concentration
- 6.2 Market Share Analysis
- 6.3 Company Profiles
- 6.3.1 Abbott
- 6.3.2 Roche Diagnostics
- 6.3.3 Siemens Healthineers
- 6.3.4 Thermo Fisher Scientific (Microgenics)
- 6.3.5 Tosoh Bioscience
- 6.3.6 Sekisui Medical
- 6.3.7 Snibe
- 6.3.8 Chromsystems
- 6.3.9 RECIPE Chemicals + Instruments
- 6.3.10 Waters Corporation
- 6.3.11 Agilent Technologies
- 6.3.12 SCIEX
- 6.3.13 Shimadzu Chemistry & Diagnostics
- 6.3.14 Bruker (Daltonics)
- 6.3.15 Zivak Technologies
- 6.3.16 Randox Laboratories
7 Market Opportunities & Future Outlook
- 7.1 White?space & unmet?need assessment
